
WHY Chris Masterjohn is WRONG ABOUT METHYLENE BLUE
Questionable studies cited

IF YOU PREFER to WATCH/LISTEN instead of READ ALL OF THIS, check out my new YouTube video on Decentralized Radio where we address this as well:
Methylene Blue has become a hot topic in the esoteric health space and biohacking community in the past few years. I think this is for good reason, as it is a very effective medicinal compound (emphasis on medicinal). Recently, the well respected Chris Masterjohn (PhD), posted a 51 page guide on Methylene Blue alongside a 2.5hr YouTube video (and a 10 min shortened overview version). You need to subscribe to his substack in order to download the 51 page guide which I did. He did a fantastic job looking at a ton of research, highlighting the mechanism of functionality, history, and side effects. I actually agree with his high level takeaway, but there is a few major points I disagree with that I will dive into here. But first, here is a brief summary of some of his perspective:
-Methylene Blue is a great treatment for malaria, pathogenic infections
-MB has shown to improve cognitive impairments such as memory/amnesia
-MB is an MAO inhibitor which leads to a “feel good” feeling from serotonin build up
-MB is beneficial for dysfunctional mitochondria
-MB can do MORE HARM than GOOD to people with functional mitochondria
-MB failed in clinical trials for Alzheimer’s treatment which raised many red flags around it’s use as a medicine
Overall: MB should be treated as a medicinal compound for what it is known to be beneficial to treat, and caution should be treated tinkering with it as a broad spectrum mitochondrial enhancement agent.
I highlighted the last two points because that is where the main contention lies for me. I think Chris was a bit ignorant in his analysis of the Alzheimer’s clinical trials and is missing context on analyzing mitochondrial respiratory chain dynamics.
Overall, I agree with his sentiment that caution should be yielded when taking Methylene Blue. I do not recommend taking methylene blue everyday or consistently for a long period of time, cycling on/off is extremely important. I also only advocate for taking low dose (5-20mg/day) which some of the research he cites seems to support. I think it should be treated as a tool for non ideal environments or health conditions, and would caution branding it as a “limitless pill” or nootropic as many have.
Alzheimer Clinical Trials
In his videos and his 51 page guide on Methylene Blue, Masterjohn highlights how “Methylene Blue Fails in Alzheimer’s”…citing an observational study from two phase III clinical trials. He also highlighted the very high dropout rate as a concern, which I will also address. Here are my main concerns with this study/clinical trial:
The compound taken WAS NOT EVEN METHYLENE BLUE
The dosage of the experimental group was 69-250mg/day
The placebo group had a dosage of 8mg/day !
The trial duration was 6-15 months of daily use

You may be shocked reading that first bullet, but for me it was no surprise because as I dove into this I recalled listening to a podcast a few months back with the real Methylene Blue expert Dr. Gonzalez-Lima, and he mentioned the issues that were ongoing in the clinical trials for Alzheimer’s treatment with Methylene Blue. The issue with Methylene Blue is that it is unpatentable since it is commercially available in its parent/true form. This is why Big Pharma will never touch it, because if it is unpatentable they can never make an ROI on it. However the research on Methylene Blue was so promising that some companies couldn’t resist. So they (TauRx) decided to make a “purified, proprietary formulation” of Methylene Blue so it could be patented and it was as “Rember®”. Rember® was used in initial trials ran between 2004 and 2007 (these are NOT the trials Masterjohn linked in his paper). The participants were given 30/60/100mg dosing. The trial had a LARGE share of controversy, and even though the 30/60mg doses showed benefits the 100mg did not and had a large amount of side effects. The trial’s blinding and methodology was highly questionable, you can read more about it HERE. '
This f*ck up led TauRx to develop another compound…a DERIVATIVE of methylene blue called Hydromethylthionine that reportedly has “better absorption into the intestine, bioavailability, and tolerability.” THIS is the compound in the study that Masterjohn is referencing, which in my research is summarized as a more stable and reduced form of Methylene Blue. My problem with Masterjohn is that no where in his paper or videos does he mention this. The studies he cites all mention Hydromethylthionine as the compound being used, NOT methylene blue or the patented original version: Rember®. Maybe Chris was just being a bit lackadaisical in his reading of these papers? I don’t think so, because Chris does very thorough work and if you read the title of the paper Methylene Blue is no where to be found and if you read the Introduction paragraph it clearly states the following:
“The most advanced late-stage program targeting tau aggregation currently in development is based on leuco-methylthioninium bis(hydromethanesulphonate) (LMTM). LMTM has recently been assigned the International Nonproprietary Name “hydromethylthionine”, recognizing it as chemically and pharmacologically distinct from methylthioninium chloride (MTC, methylene blue).”
Why is this a big deal? Because Hydromethylthionine is NOT methylene blue. The research states clearly that it is chemically distinct, and according to my research is a more reduced form. Met. Blue is a positively charged compound, so if you are reducing it to a neutral or negative charge, you are fundamentally changing its ability to donate/accept electrons in our biology. It is more similar to the standard reduced form of Methylene Blue: Luecomethylene Blue (AKA Methylene White).
Overall I am not a biochemistry expert like Masterjohn may be, but I trust the opinion of the true Methylene Blue expert Dr. Gonzalez-Lima (who performed a lot of the beneficial research for MB) when he mentioned these trials were NOT the right way to show MB is beneficial for AD treatment. I would question Masterjohn on why he would leave out the fact that the compound used in the studies he linked was not actually Methylene Blue, but a derivative. Was he trying to hide that or was he just assuming it meant nothing and the results should have been the same and since they were similar to the Rember® results it did not matter. Regardless, important to specify. I still respect Chris and his work tremendously.
BACK TO THE TRIALS and points 2-4. Dosing. 250mg/day is way beyond the minimal threshold dose that anyone in the esoteric health or biohacking community would recommend. In his interviews Gonzalez-Lima is CLEAR that MB becomes pro-oxidant, losing anti-oxidant at a certain threshold. I think most of the research says that it is closer to 5mg/kg, which is still far higher than the 250mg/day dose…but it WAY closer to the “threshold” for pro-oxidant behavior compared to the minimal effective dose. How do we know that? Well there are many low dose MB studies far under 1mg/kg that show beneficial effects. And THE PLACEBO group in the clinical trial was given 8mg/day to help with the blinding issue since MB turns your pee blue/green. The result? The placebo had just as beneficial effects as the experimental group…LOL.
It is clear from these trials that 100+ mg/day of these compounds is not beneficial. The trials noted that the minimal threshold dose was far lower for Hydromethylthionine compared to MB. The other thing Masterjohn harped on was that the benefits of taking the compound plateaued halfway through the trial and that the side effects were really bad. Remember, these folks were taking Hydromethylthionine daily for 6-15 months (!!). I am treating this as if it were MB being taken here, in which I would never recommend or know anyone who recommends taking it every single day for 6+ months. MB has numerous benefits, but it is a medicinal compound at the end of the day. All medicinal compounds come with side effects, and MB is not short of that. In these Alzheimer’s studies, the diminishing returns found after many months of use just proves the fact that you should not be taking MB or its derivatives every single day for a prolonged period of time, especially at dosages of 100-250mg! Amongst many knowledgeable friends and practitioners in the health space, ALL recommend cycling MB on and off. The longest one should consider taking every single day is 30 days for TBI or PCOS recovery and then take a full 30 days off. Many recommend even shorter on/off periods such as 5 on/ 2 off, 7 on / 7 off, etc. THIS IS NOT MEDICAL ADVICE and I can tell you that personally I have never taken MB more than 2-3 days in a row and that was when I was traveling from US to Europe.
For this reason, I discount the fact that there were a lot of side effects in the Alzheimer’s studies, because 1) the dosing and dose period was FAR too high and long AND 2) they were being compared to the placebo group who had the real minimal effective dose! Chris Masterjohn cites that the experimental group had 5.6x greater instance of injuries from falls compared to the placebo, but does not consider that the placebo is not indicative of a normal population since they were receiving 8mg/day. It is very plausible that the 8mg/day was reducing the number of injuries from falls in study group. No one can say for sure, but at the end of the day these Alzheimer’s studies are about as good as garbage for determining the efficacy and safety of Methylene Blue.

MB can do MORE HARM than GOOD to people with functional mitochondria
The other main point Chris Masterjohn makes in his 51 page guide and videos is that based on the research, Methylene Blue can benefit people who have dysfunctional mitochondria, but taking it when you don’t have any mitochondrial dysfunction can actually harm you or make your mitochondria less efficient. This is a bit controversial in my opinion, especially after doing a lot of research on mitochondrial dynamics in the past few months, and to give you the TLDR, I personally don’t think we have a good enough understanding or research about Methylene Blue or the mitochondria to make this conclusion.
Before we dive in, I want to say however that this is a conservative and pretty justified conclusion for Masterjohn to make at a high level, because it urges caution to be using MB as a biohacking substance. I do agree with him that MB provides more benefit to those who need it, but I am debating the mitochondrial dynamics side of things here.
Chris cites MB is helpful for those who have dysfunctional mitochondria, but isn’t that everyone?
Here’s the thing that gets me with Chris’s prognosis about MB being harmful for people who don’t have mitochondrial dysfunction…EVERYONE DOES (to some degree). In todays modern toxic soup world, our mitochondrial are being bombarded from all directions. Unless you live in the remote wilderness with no nnEMFs or artificial light, eat perfectly pristine food, and avoid all other environmental toxins (heavy metals, glyphosate, parabens, microplastics, etc.), then you have SOME mitochondrial dysfunction. The rate and severity is what differs person to person. If you have strong circadian health and melatonin production, then you have proper mitochondrial dynamics in which mitophagy and apoptosis will occur so your body can clean up and repair damaged mito. If you have chronic dysfunction, your mito will mutate its mtDNA and result in heteroplasmy. A high heteroplasmy rate leads to ALL chronic disease according to mitochondria research expert Dr. Doug Wallace. So what I am saying is that you COULD easily argue that MB has a use case for MANY if not all our population to some degree. Being more generous to Chris, I personally only take it when I know I am encountering severe oxidative stress that can lead to mitochondrial dysfunction (ie: traveling, injury, toxin exposure, sickness, hypoxic environment, extreme exercise recovery, etc.).
Studies that Masterjohn cited do not share his opinion
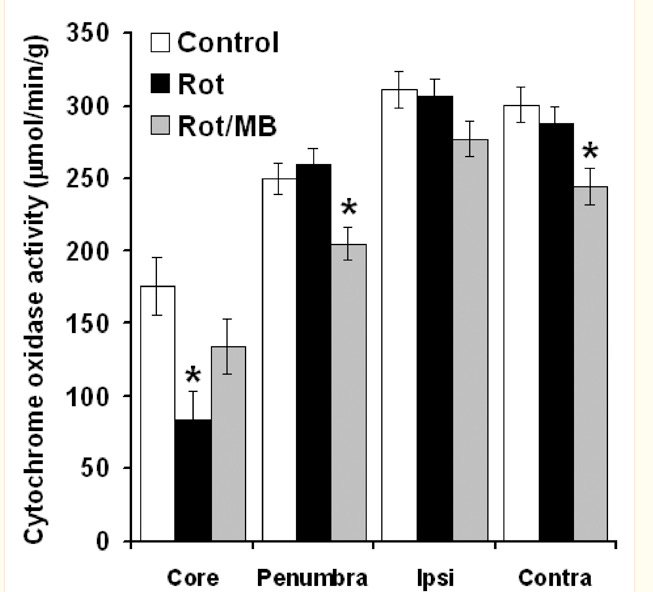
In his 51 page report on MB where he dives into the compound doing “more harm than good” for functional mitochondria, he cites 3 studies. The first one I could not access but was very curious on the dosing. The second study injected rats with a known mitochondrial toxin “rotenone” and then administered MB to see how mitochondrial activity would recover. Cytochrome C Oxidase activity (Complex IV) was measured as the determining factor of “metabolism”. MB did rescue CCO activity in the region that was injected with rotenone (the lesion core), but in the other areas of the brain as Masterjohn highlights, MB caused a drop in CCO activity. This does seem like a warranted point, but then in the third study that Masterjohn cites, a similar thing occurred when rats had sodium azide injected (CCO inhibitor), but with a different twist. The rats injected developed amnesia, but then were administered MB and actually returned to better memory than the control group. Despite this, CCO activity was actually even lower after the MB compared to just after the sodium azide injection. This is likely due to MB completely bypassing and reconfiguring the ETC, which Masterjohn does acknowledge. However, Masterjohn goes on to highlight how MB decreased significantly the intrinsic connectivity of visual motor loop networks…which to him is a concern and potential reason that the Alzheimer studies showed high incidence of injuries from falls (albeit being a derivative of MB, not MB remember).
This is where I get kind of taken aback by Masterjohn’s perspective. In the paper they highlight MB working as kind of a rerouting mechanism where it is focusing the attention on the incident of injury. Masterjohn even highlighted this as mentioned by the authors as “adaptive reconfiguration”, but he didn’t buy it. Fair game to Chris for his opinion, but to me I have recently learned about the great nuances of mitochondrial dynamics and the ability for our mitochondria to re-organize for the benefit of efficiency given the environment they are in. I think it seems like that MB could be acting in a similar manner, but we cannot know for sure…and this is why I think it is premature to assume that MB is “BAD” for folks who don’t need it.
Not following what I am getting at? Chris goes on in his 51 page guide to mention known mitochondrial toxins, in which he mentions both Berberine and Metformin as Complex I inhibitors. You may be aware that both Berberine and Metformin are fantastic for blood sugar management and the treatment of diabetes. That is not by coincidence in regards to its inhibition of Complex I. Carbs (glucose) produce far higher activity of Complex I compared to Complex II (where fats produce a higher ratio of activity via higher FADH2:NADH). Perhaps compounds like Metformin act in inhibiting Complex I, which then generates Reactive Oxygen Species (ROS) via Reverse Electron Transport (RET) in a similar manner to when our body oxidizes a high amount of fatty acids (high FADH2:NADH) to upregulate Complex II activity. Sounds crazy? ROS are only bad right? Read this study to open your mind (if you want to nerd out a bit).
I know Chris is a nutrition expert, and I really do respect his work but at the end of the video when he mentioned “simple mitochondrial hacks” such as eating more carbs for a downregulated Complex I and eating more fats for a downregulated Complex II I almost burst out into laughter. THIS GUY IS SO SMART yet understands nothing about dietary seasonal context. Why do you think that high oxidation of fatty acids results in RET ROS signaling at Complex I? Is it maybe that our mitochondria are sensing a lower carb intake in the environment, coupled with the light input to signal that winter is coming and adaptation is needed to burn fats more efficiently? No, it couldn’t be that. It couldn’t be possible that this RET ROS signal from a high FADH2:NADH ratio could lead to a re-organization of the electron transport chain into something MORE EFFICIENT…say a supercomplex formation…
That is exactly what happens. AND that is why Chris Masterjohn misses the context of mitochondrial dynamics and adaptation. MUCH more coming on this topic, because it is truly fascinating and solidifies why embracing seasonality is so important + highlights the importance of ROS as a signaling mechanism.
All of this research is very new, so we are only cracking the tip of the mitochondrial dynamics iceberg. Chris Masterjohn is in the nutrition silo. He is a wizard of micronutrients, but I challenge him to reconsider his stance on mitochondrial dynamics and methylene blue.
Albeit, I do agree with him that we should all be yielding caution and NOT ever taking MB daily.
This was a fun rant, and I will be doing less frequent, deeper dive posts on substack going forward. It is time to get you all educated on what matters.
Learn alongside me and always…
Stay Sovereign,
Tristan
Very informative "rant". I hope you can dive deeper into this, and "explain it like I'm five".
Thank you!
Other than Dr. Gonzalez-Lima are you familiar with other experts who have studied methylene blue. I would recommend Dr. Scott Sherr, The Riordan Clinic, Dr. Lewis Clarke (Clarke Neuroscience), Dr. Joe Mercola, Dr. Mobeen Syed (he discusses MB in 3 or so of his Dr. Been series), and Dr. Steve Warren. I have done a very deep dive into MB, and in particular MB combined with photobiomodulation (red light therapy). In low doses 7.5-20 mg daily I think it is completely safe. Dr. Mercola has done an excellent interview with Dr. Gonzalez-Lima I highly recommend. Dr. Kan Cao discovered the benefits of MB for the skin while conducting research into treatment for progeria while working at NIH. Interesting stuff.